Evaluation Finds Significant Quality Improvements in Independent Practices Across Los Angeles
January 13th, 2026
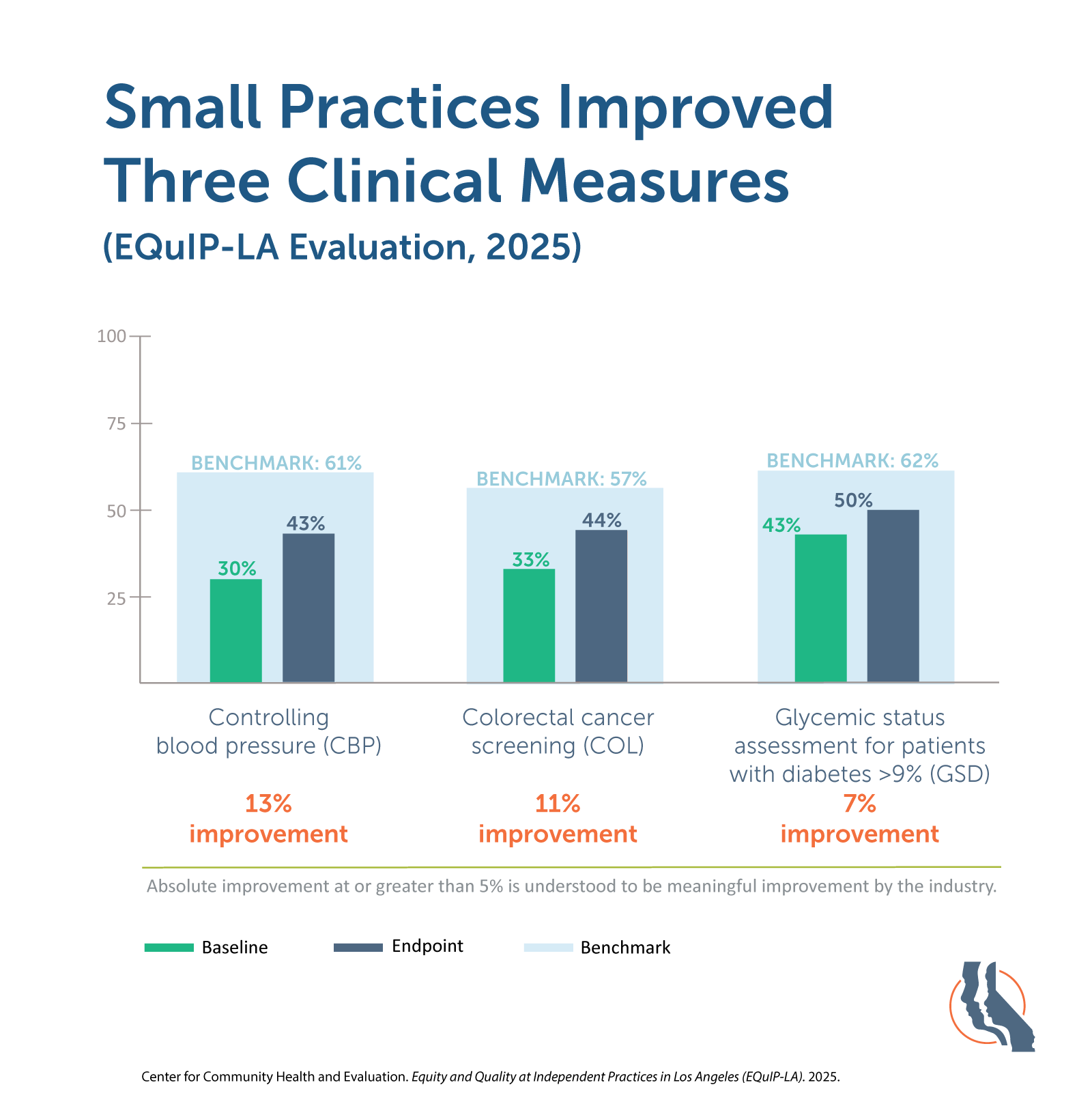
Findings show measurable improvements in diabetes, hypertension and colorectal cancer screening
Oakland, CA, January 13, 2026 – An independent evaluation shows that small medical practices serving Los Angeles’ most underserved communities achieved 7 to 13 percent improvement in blood pressure control, cancer screening and diabetes care. The findings come from the Equity and Quality at Independent Practices in Los Angeles (EQuIP-LA) initiative, which partnered with 31 independent practices to strengthen care quality for Medicaid patients across the region.
The EQuIP-LA initiative was led by the California Quality Collaborative (CQC), a health care improvement program that partners with providers, health plans and the delivery system across the state to strengthen primary care, advance health equity and spread evidence-based quality improvement. Through EQuIP-LA, CQC supported participating practices with a comprehensive technical assistance approach that included direct funding, targeted training, personalized advising, data insights and collaborative learning. CQC has supported hundreds of practices statewide through evidence-based improvement programs.
The evaluation, conducted by the Center for Community Health and Evaluation (CCHE), found statistically significant improvements (p<0.01) across all three priority clinical quality measures, with 30 of 31 practices improving at least one measure. Practices also reported strengthened foundational capabilities, increased readiness to sustain quality improvement and a deeper understanding of how to identify and address disparities in their patient population.
“This evaluation confirms what we see every day,” said Peter Robertson, Director of Practice Transformation at CQC. “Independent practices are cornerstones of care for Medi-Cal patients, and when we invest in their capacity, the entire health system benefits. These results show that meaningful improvement is not only possible but within reach for practices across California.”
Key findings from the evaluation include:
- Improved clinical outcomes: Participating practices achieved 7 to 13 percent improvement in blood pressure control, colorectal cancer screening and glycemic assessment, with 30 of 31 practices improving at least one measure.
- Strengthened primary care capabilities: Practices reported gains across CQC’s seven foundational domains of primary care, including team-based care, data-driven improvement and leadership engagement.
- Enhanced capacity for improvement: Providers and staff reported increased confidence in their ability to apply quality improvement methods and sustain improvements beyond the initiative.
- Equity-focused change: Practices deepened their understanding of health equity concepts and adopted strategies to better identify and address disparities within their patient populations.
“EQuIP-LA helped our practice strengthen how we deliver care for our patients. By training medical assistants as community health workers and using patient registries to guide outreach, we were able to close gaps in care and better connect patients to the medical and social services they need,” said Dr. Mallu Reddy, founder and medical director of Reddy Care Medical.
Building on lessons from EQuIP-LA, CQC continues to support care teams through training and applied learning opportunities, including its Improvement Coaching Workshop. The workshop offers participants hands-on training with core quality improvement tools that helps them advance real projects within their organizations. The training includes a pre-session orientation, full day of collaborative learning and post-session support. Registration for the April 2 session in Los Angeles is now open.
EQuIP-LA was funded by the California Health Care Foundation, which works to improve the health care system so that all Californians have the care they need.
Supporting Media Assets
About California Quality Collaborative (CQC)
The California Quality Collaborative (CQC), a program of the Purchaser Business Group on Health, is dedicated to improving the quality and affordability of health care across California. CQC collaborates with health plans, providers and purchasers to drive systemwide transformation and promote high-value, patient-centered care.
About the Center for Community Health and Evaluation (CCHE)
The Center for Community Health and Evaluation (CCHE) designs and evaluates health-related programs and initiatives across the United States. Its mission is to improve the health of communities with collaborative approaches to planning, assessment, and evaluation. CCHE is part of Kaiser Permanente Washington Health Research Institute.
Media Contact:
Anna Elgart
California Quality Collaborative
Purchaser Business Group on Health
415-615-6322
aelgart@pbgh.org
Strengthening Care Where It Matters Most: What We Learned From EQuIP-LA
December 9th, 2025
Small independent practices are essential to California’s health care safety net. They provide trusted, community-based care to millions of patients, yet they often have fewer resources to develop the quality improvement (QI) and data capabilities needed to meet today’s health care demands.
A new independent evaluation of the Equity and Quality at Independent Practices in Los Angeles (EQuIP-LA) initiative shows what’s possible when these practices receive targeted support. EQuIP-LA (2023-2025) provided funding, individualized coaching and hands-on technical assistance to 31 independent practices that collectively served more than 50,000 Medi-Cal enrollees.
The evaluation, conducted by the Center for Community Health and Evaluation (CCHE), found that participating practices made meaningful gains in clinical quality, strengthened foundational primary care capabilities and increased their ability to sustain improvement over time.
EQuIP-LA was funded by the California Health Care Foundation.
What the Evaluation Found
Significant improvement in priority clinical measures
Across the two-year initiative, practices demonstrated statistically significant improvements in three priority areas: controlling blood pressure, colorectal cancer screening and glycemic status assessment for patients with diabetes. Almost every practice improved at least one clinical measure, and more reached national performance benchmarks by the end of the program. Practices credited strategies such as proactive patient outreach, documentation improvements and use of at-home screening kits.
Stronger advanced primary care capabilities
Practices also saw gains across most of the seven foundational domains of primary care, including engaged leadership, team-based care and data-driven improvement. Many achieved the maximum score in one or more domains and reported increased confidence in sustaining new workflows and participating in future QI programs.
Coaching improved infrastructure across the ecosystem
Through EQuIP-LA’s community-based coaching model, four provider organizations strengthened their internal coaching, data reporting and QI support infrastructure. These organizations plan to continue coaching and partnership with practices beyond the grant period.
Health equity embedded throughout
EQuIP-LA integrated equity into every component of the program, from intentionally recruiting practices serving diverse communities to supporting data stratification, patient-family engagement and outreach tailored to population needs. Participants reported increased understanding of equity concepts and early steps toward operationalizing these practices.
“CQC has helped us by providing a lot of useful [health equity] tools and resources that we didn’t have before in working with practices and explaining these things to them.”
— Participant, provider organization
Why This Work Matters
Independent practices care for many of California’s most underserved communities. The EQuIP-LA evaluation shows that when practices receive time, tools and tailored support, they can achieve meaningful improvements in quality and build the capabilities needed for long-term change. These findings reinforce the importance of investing in the places where patients already receive care and where trusted relationships are strongest.
“Independent practices are cornerstones of care for Medi-Cal patients, and when we invest in their capacity, the entire health system benefits,” said Peter Robertson, Senior Director of Practice Transformation at the California Quality Collaborative. “These results show that meaningful improvement is not only possible but scalable across California.”
These results tell a powerful story about impact, and the practice experiences behind them offer an even deeper look at what change required.
Explore More Stories From EQuIP-LA
Want to see how practices put these strategies into action? Explore additional stories and firsthand insights from EQuIP-LA participants:
Video Features
Implementation Spotlights
These resources offer a closer look at the approaches, challenges and innovations that contributed to the program’s success.
Access the full evaluation here and discover more about EQuIP-LA.
CQC Releases New Building Resiliency Toolkit on CA Path
August 25th, 2025
Health care teams face constant change—from shifting policies to new delivery models and the everyday challenges of patient care. To support frontline providers and care teams in navigating these demands, the California Quality Collaborative (CQC) has released a new Building Resiliency Toolkit, now available through California’s PATH On-Demand Resource Library.
About the Toolkit
The Building Resiliency Toolkit is a self-paced resource designed to help individuals and teams strengthen their ability to adapt, recover and thrive in the face of challenges. Through five sequential modules, participants will learn practical strategies to:
- Define and assess resiliency at the individual, team and organizational level
- Build confidence in leading through change and addressing resistance
- Apply adaptive leadership skills to complex, real-world challenges
- Improve communication strategies to embody and sustain change
- Establish accountability and embed resiliency practices into everyday work
Each module combines key concepts with practical tools and examples, giving health care professionals the knowledge and confidence to foster resilience in themselves and their teams.
Why It Matters
Burnout and stress are persistent challenges across the health care workforce. Building resiliency is about more than “bouncing back.” It means cultivating the confidence and skills to adapt to change, stay grounded under pressure and create sustainable practices that prevent fatigue. By investing in resiliency, organizations can strengthen team performance, support staff well-being and improve patient care.
Practical Support for Providers Through TA Path
The Building Resiliency Toolkit is part of CQC’s broader contribution to the Providing Access and Transforming Health (PATH) Technical Assistance (TA) Marketplace, led by the California Department of Health Care Services. As an approved TA vendor, CQC brings deep expertise in:
- Promoting Health Equity. Helping provider organizations embed equity into care delivery with culturally responsive models and equity-focused quality improvement methods.
- Strengthening the Workforce. Supporting recruitment, retention, and advancement strategies that build inclusive, resilient and mission-aligned teams.
- Maternal Health and Pediatrics. Improving care models and outcomes for pregnant and postpartum individuals and children, recognized priority areas in TA Path.
Through TA Path, CQC is partnering with providers and delivery organizations to embed health equity into care, strengthen the frontline workforce and develop sustainable models that meet the needs of Medi-Cal members. Resources like the Building Resiliency Toolkit represent just one-way CQC is equipping organizations with practical tools to drive meaningful change.
Accessing the Toolkit and Other Resources
The Building Resiliency Toolkit is available now through the CA Path website as part of its On-Demand Resource Library, which provides static resources for organizations at all levels of readiness, including those engaged in Enhanced Care Management, Community Supports and Justice-Involved
Turning Shared Goals Into Real-World Results: CQC’s 2024 Impact
August 5th, 2025
Across California, the challenges facing our health care system remain significant—but so do the opportunities for transformation.
At the California Quality Collaborative (CQC), we believe real change happens when payers, providers, community partners and patients come together around a common purpose: better health outcomes, more equitable systems and stronger primary care.
In 2024, CQC’s programs touched more than 932,000 Californians through technical assistance and multi-stakeholder alignment efforts. This included helping practices implement new payment models, expand behavioral health integration, support youth behavioral health and embed equity into core quality improvement efforts.
2024 Highlights
From convenings and coaching to collaborations and tools, CQC’s work in 2024 helped build a stronger, more equitable delivery system for Californians across the state.
Explore the full 2024 Impact Report
Driving Access Through Innovation: Tweedy Medical Group’s Story
June 3rd, 2025
Primary care providers are often the first line of defense against preventable health issues, but many face systemic barriers that limit their ability to support patients fully. At Tweedy Medical Group in Los Angeles, cost was one of the biggest challenges. For Medi-Cal patients, high medication copays too often meant leaving the pharmacy empty-handed
Watch the video above to see how Tweedy Medical Group removed cost barriers and strengthened patient outcomes with support from CQC’s Equity and Quality at Independent Practices in LA County (EQuIP-LA) collaborative.
By launching a nonprofit and partnering with a local pharmacy, the clinic found a sustainable solution: cover unaffordable copays for Medi-Cal patients and ensuring continuity in care. The result was improved blood pressure control, fewer emergency department visits and greater patient trust.
Participation in EQuIP-LA helped validate and expand these efforts by connecting Tweedy Medical Group to a statewide network of peer clinics, real-time data insights and targeted quality improvement coaching.
“For the longest time we just felt like no one cared about us as a clinic. But with EQuIP-LA, we finally had support and a way to connect with the larger health care system—and that pushed us to do even more.”
— Dr. Robert Hernandez, Tweedy Medical Group
About EQuIP-LA
Launched in 2023, EQuIP-LA was a two-year improvement collaborative led by CQC dedicated to reducing disparities of care experienced by Medi-Cal enrollees of color. This work was made possible through the generous support of the California Health Care Foundation and in partnership with Health Net and L.A. Care Health Plan. Learn more.
Closing Gaps and Centering Equity: Reddy Care Medical’s Story
May 7th, 2025
Primary care practices play a critical role in closing equity gaps—especially when supported by improvement efforts designed with community needs in mind. That’s the approach behind Equity and Quality at Independent Practices in LA County (EQuIP-LA), a two-year quality improvement collaborative led by the CQC to reduce disparities of care experienced by Medi-Cal enrollees of color.
Watch the video above to hear how Reddy Care Medical strengthened care coordination and patient follow-up through EQuIP-LA.
Serving patients in Los Angeles County, Reddy Care Medical utilized EQuIP-LA’s community-based coaching model to support lasting improvements in chronic disease management and preventive care. Their efforts focused on addressing equity barriers for Medi-Cal patients, many of whom had previously faced challenges navigating the health system or accessing timely care.
The practice’s story underscores how locally grounded support, including tailored coaching and actionable data insights, can empower teams to embed equity into day-to-day workflows. Reddy Care Medical’s progress reflects the broader goals of EQuIP-LA: enabling sustainable improvements through community partnership, patient-centered strategies and real-time quality improvement tools.
“Most practices we met had this idea that we are treating patients equally. But there’s a difference between equal and equity. Because are you able to meet all the patients where they are?”
— Lydia Muse, Community-Based Coach, EQuIP-LA
About EQuIP-LA
Launched in 2023, EQuIP-LA was a two-year improvement collaborative led by CQC dedicated to reducing disparities of care experienced by Medi-Cal enrollees of color. This work was made possible through the generous support of the California Health Care Foundation and in partnership with Health Net and L.A. Care Health Plan. Learn more.
Transforming Medicare in California: Pathways to Improvement
March 20th, 2025
By 2030, nearly one in five Californians will be 65 or older, and the majority of them will be Medicare beneficiaries with complex health care needs. To address these evolving challenges, the California Quality Collaborative, The SCAN Foundation, Archstone Foundation, Gary and Mary West Foundation with partnership from the Department of Health Care Services Office of Medicare Innovation and Integration launched the California Medicare Collaborative (Collaborative) in March 2024. This year-long, multi-stakeholder effort was dedicated to improving care for residents insured solely by Medicare, including duals, non-duals and those in both traditional Medicare and Medicare Advantage programs.
Strategic Design and Implementation
The Collaborative’s approach was built on a foundation of multi-stakeholder engagement, drawing together state leaders, health care providers, health plans, advocacy groups and others. This collective effort focused on initiating change within the existing regulatory framework to quickly implement strategies that could have a short- to medium- term impact on the health care landscape. The initiative targeted four key areas:
- Chronic Illness Management and Care Coordination
- Access, Equity and Disparities in Care
- Beneficiary Choice in a Confusing Market
- Cognitive and Behavioral Health
Each area was carefully chosen to address the comprehensive needs of the senior population and to pioneer changes within California’s Medicare landscape.
Health Care Industry Recommendations
The Collaborative developed targeted recommendations to drive systemic improvements.
Strengthen Chronic Illness Management and Care Coordination
- Strengthen chronic care management via supportive funding streams and payment policy.
- Promote Advanced Primary Care (APC) by investing in supportive training, clinical care models and compensation models for Medicare patients.
- Increase support for and coordination with organizations that address patients’ health related social needs (HRSNs) via capacity building and innovative payment models.
Enhance Access and Equity
- Improve population health management by improving data on Medicare beneficiary HRSNs and evaluating programs that seek to meet those needs.
- Increase access to care for special populations—including low-income Medicare beneficiaries, Medicare beneficiaries with limited English proficiency, those receiving Medicare because they are on social security disability, and those that live in rural communities—via effective care delivery models.
- Strengthen the clinical workforce needed to serve Medicare beneficiaries in an equitable way through training for the current workforce, care team diversification and supports for trainees in shortage professions.
Improve Beneficiary Decision-Making
- Strengthen the clinical workforce needed to serve Medicare beneficiaries in an equitable way through training for the current workforce, care team diversification and supports for trainees in shortage professions.
Improve screening and supports for Cognitive and Behavioral Health
- Reduce stigma and normalize seeking cognitive and behavioral health services via culturally competent messaging and channels.
- Amplify and improve screening to promote earlier and wider detection of cognitive and behavioral health needs via spread of existing training resources and care models.
- Increase supports for patients with cognitive and behavioral health needs and their caregivers by expanding access to navigation and wrap-around services.
Conclusion and the Road Ahead
The Collaborative’s work represents a solid way forward in the state’s efforts to adapt its health care system to better meet the needs of its aging population. By focusing on strategic, actionable recommendations, The Collaborative aims to not only improve the quality of care but also ensure that all Medicare beneficiaries in California have access to the services they need to lead healthier, more fulfilled lives.
For a more comprehensive exploration of these strategies and detailed recommendations, access the full issue brief here.
Strengthening Health Equity through Primary Care Transformation
October 25th, 2024
Primary care serves as the cornerstone of health care delivery, especially when addressing long-standing disparities in access and quality. To fully realize its potential in advancing health equity, the California Health Care Foundation (CHCF), in collaboration with Mathematica, highlights the importance of investing in primary care through a new report. The report emphasizes that while primary care is critical, underfunding and systemic barriers continue to limit its effectiveness.
To change this, key stakeholders, including providers, health plans and purchasers, must focus on actionable steps to improve care access, quality and equity.
California Advanced Primary Care Initiative
The CHCF report cites the California Advanced Primary Care Initiative as a prime example of how collaboration among health plans, providers and purchasers can successfully address health inequities. Launched by the California Quality Collaborative (CQC) and the Integrated Healthcare Association, the initiative aims to redefine primary care by focusing on high-value care that is accessible, coordinated and patient-centered. The initiative sets clear goals to improve quality, reduce costs and target disparities in underserved populations.
The California Advanced Primary Care Initiative offers a model that includes:
- Enhanced access to care. Expanding access through same-day appointments, telehealth integration and extended clinic hours, especially in underserved areas.
- Whole-person care. Integrating behavioral health services within primary care to address both mental and physical health, which is especially important for underserved communities facing multiple health challenges.
- Care coordination. Streamlining coordination between different providers — primary care, specialty and hospital care — to ensure smoother transitions and continuity for patients with chronic conditions.
Recommendations for Health Care Industry Stakeholders
The CHCF report offers the following recommendations for providers, health plans and purchasers:
-
For Health Care Providers
- Integrate behavioral and social services. Embed behavioral health and social care within primary care to address complex patient needs.
- Expand access. Increase telehealth options, same-day appointments and extend hours to reach underserved communities.
- Ensure continuity of care. Focus on building long-term patient-provider relationships and better care coordination to improve outcomes.
-
For Health Plans
- Increase primary care investment. Allocate more resources to primary care, addressing its critical role in population health.
- Adopt value-based payment models. Implement payment models that reward providers for improving patient outcomes and reducing disparities.
- Enhance data collection. Improve data on patient demographics and social determinants to better target health interventions.
-
For Purchasers
- Support primary care funding. Advocate for increased spending on primary care services within health plans.
- Address social determinants. Focus on housing, food insecurity and transportation, working with providers and health plans to mitigate these factors.
- Leverage accountability tools. Use tools like the Health Value Index to ensure resources are effectively allocated to primary care and equity initiatives.
Learn more about the California Advanced Primary Care Initiative.
Pain, Perseverance and Patience: Michelle’s Story
June 4th, 2024

Michelle with her daughter Vonyae
In early 2022, Michelle Rosser, a Los Angeles resident and mother of three, began to experience persistent pain and discomfort. Concerned about her worsening symptoms, she sought medical care, marking the beginning of a challenging journey through the health care delivery system. Further examinations revealed multiple health issues, including high blood pressure and chronic pain, leading to a complex path of appointments, referrals and miscommunications.
Initial Diagnosis and the Struggle for Proper Care
Michelle’s health concerns required numerous appointments, tests and referrals, highlighting the fragmented nature of the health care system. Michelle’s chronic pain, high blood pressure and weight management issues compounded her challenges. “I have two bad hips now, not just one. I had to wait three months to go to physical therapy,” she said. The delays in receiving appropriate care and referrals left Michelle feeling stuck and discouraged.
The Pain of Navigation and Lack of Support
Navigating the health care system was a daunting task. “It takes a long time to get an appointment,” Michelle said. She describes feeling as though her concerns were not taken seriously and that she lacked information to support her care. “I needed an MRI in order to get a referral for pain management for my back. That was the missing piece throughout a year that had passed by.”
The lack of proper communication and follow-through left Michelle feeling neglected and unheard, and exacerbated her physical and mental health struggles. “I kind of got lost in my mental health,” she says, reflecting on the additional strain her health struggles placed on her emotional well-being. The constant battle to get the care she needed only intensified these mental health issues, creating a cycle that was hard to break.
Embracing Patient Feedback: A Turning Point
Michelle experienced a significant improvement in her health care experience after completing a patient feedback survey from her health plan. “I got a flier in the mail so I filled it out. When they [Michelle’s health plan] got involved, everything came into play — I got the referrals, I got to see my doctor,” she recalled. Being given a channel to be heard, advocate for herself and provide valuable feedback to her health plan about her experience helped shape her care plan, becoming a turning point for Michelle — illustrating the power of patient feedback mechanisms and their ability dramatically enhance health care services.
Finding Community and Advocacy
While seeking community resources, Michelle connected with the California Quality Collaborative’s Equity and Quality at Independent Practices in LA County (EQuIP-LA), a quality improvement collaborative for small, independent primary care practices and IPAs serving Medi-Cal enrollees of color in Los Angeles County. Joining the EQuIP-LA Steering Committee reflects her commitment to her community and her health. “Each time when I go back to the doctor I think about a question from the last committee meeting and then I have an answer,” said Michelle, illustrating how her involvement has influenced her health care approach.
Michelle’s journey is ongoing, but her outlook remains hopeful, “Patience worked for me and staying connected to the health care system while allowing it to work,” she said. She continues to work toward her health goals, including weight management, lifestyle changes and mental health. Her story is a testament to the strength and resilience of patients, underscoring the need for a more supportive and efficient health care system.
Equity and Quality at Independent Practices in LA County
The EQuIP-LA improvement collaborative is dedicated to improving health outcomes and reducing disparities of care for Medi-Cal enrollees of color across Los Angeles. The collaborative supports 31 small, independent primary care practices and independent physician associations (IPAs) with technical assistance that addresses:
- Multi-stakeholder collaboration. Aligning health care providers, IPAs, payers, community-based organizations and patient advocates to support comprehensive care and address disparities.
- Capacity building. Providing funding, training and technical support to IPAs and practices to implement and sustain disparities reduction programs. EQuIP-LA uses community-based practice coaches, guided by CQC improvement advisors, to support change interventions.
- Patient engagement and advocacy. Emphasizing the importance of patient feedback and involvement to ensure responsive and patient-centered care.
- Data-driven approach. Using data and evidence-based frameworks to identify improvement opportunities and measure impact on health outcomes.
Learn more about EQuIP-LA.
A Journey of Resilience and Advocacy in a Complex Health Care Landscape
April 17th, 2024
In early 2015, during a routine doctor’s appointment, David Ford’s physician recommended a colonoscopy. However, it wasn’t until three months later, when Ford, a senior government relations manager with Southern California Edison, experienced rectal bleeding on his way to work, that the urgency of his situation became apparent. An emergency surgery revealed a tumor on his intestines, leading to a diagnosis of colorectal cancer — the second leading cause of death from cancer in the United States.
Navigating the Delivery System
Ford was thrust into a challenging health care journey, facing the intricacies of cancer treatment. Navigating the health care system added another layer of complexity. Ford had to coordinate appointments across different health care providers, understand the nuances of his insurance coverage and make informed decisions about his treatment options. The difficulty of this process was exacerbated by the need to decipher medical jargon and understand the implications of different medical procedures and tests.
Throughout his treatment, Ford, a Black man, became acutely aware of the disparities in health care access and the additional challenges faced by those in minority communities. Black Americans have a 20% higher incidence of colorectal cancer and a 40% higher death rate from the disease than white Americans, underlining the urgent need for action to reduce these inequities. During a recent California Quality Collaborative (CQC) webinar that explored disparities in colorectal cancer care, Ford shared his story, recounting his delay in undergoing a colonoscopy and how his experience may have been different had he been more proactive about undergoing the screening test.
During an annual physical exam in 2018, Ford’s physician conducted a test that revealed elevated prostate-specific antigen numbers, leading to a diagnosis of prostate cancer. After undergoing radiation treatment, he was able to make a full recovery. Ford’s experience underscores the critical need for proactive health management and screening for early detection through tools such as the EpiSwitch Prostate Screening (PSE), especially in communities of color, where distrust in the health care system and barriers to accessing care are common.
A Voice for Advocacy and Change
Today, Ford serves as a member of the Cancer Action Network board, actively engaged in lobbying and advocacy efforts. His experience has fueled his commitment to cancer research, funding and policy change, making him a vocal advocate for equitable access to care.
“There’s more advocacy and education to do through outreach and connection with community-based groups, churches and national organizations to get behind this campaign because I do think that this is a civil rights crisis, particularly in the African American community,” said Ford. Ford emphasizes the importance of early detection, especially given today’s innovative technology and testing options which are less invasive and allow for greater accuracy: “Cancer is much easier to treat and deal with if it’s early… get in to see someone as soon as possible when you think something is wrong.”
Strategies to Combat Colorectal Cancer Disparities
The following key strategies can help reduce disparities in colorectal cancer care within the delivery system:
- Multi-stakeholder collaboration. Alignment among health care providers, payers, policy makers and patient advocates is essential for comprehensive care and disparity reduction.
- Patient engagement and advocacy. Engaging patients in their health care journeys, especially through preventive measures like cancer screening, is critical for early detection and treatment.
- Research and data utilization. Utilizing comprehensive data and research findings to informs policy and practice, leading to more effective screening and improved health outcomes.
- Community outreach and education. Developing community-based programs and partnerships facilitates access to screening and treatment services, building trust and awareness within communities.
CQC is working to advance health equity through programs like Equity and Quality at Independent Practices in LA County, a quality improvement collaborative for primary care practices and independent physician associations focused on reducing health disparities for Medi-Cal enrollees of color.
To learn more about disparities in colorectal cancer care and what patients, providers, health plans and purchasers can do to advance equitable care, view a recording of CQC’s latest webinar Addressing Disparities in Colorectal Cancer and access our guide to designing an effective colorectal cancer outreach campaign.
Empowering Care: The Role of Alternative Payment Model Design in Advancing Equity
January 25th, 2024
Alternative Payment Models (APMs), incentivizing clinicians to provide high-quality, cost-efficient care beyond traditional fee-for-service payments, hold immense potential to revolutionize health care delivery, expanding access, improving outcomes and addressing health disparities. However, to unleash their transformative power, APMs must be thoughtfully designed to prioritize health equity and mitigate unintended negative consequences. Factors such as poverty, institutional racism, education, economic opportunities, insurance coverage and the living environment significantly influence health equity. When capitated payments and performance incentives fail to account for the necessary resources to provide adequate care, practices serving populations with higher medical and social risks may face financial challenges, ultimately impacting health outcomes negatively.
Multi-Stakeholder Alignment
Multi-stakeholder collaboration is pivotal in aligning the design and implementation of a payment model that champions health equity. Through the California Advanced Primary Care Initiative, California Quality Collaborative (CQC) and partner Integrated Healthcare Association (IHA) bring together health care payers to collectively strengthen primary care delivery. The initiative aims to facilitate the delivery of high-performing, value-based care, reducing costs while enhancing quality and equity. CQC and IHA collaborated with health plans to develop a common hybrid primary care payment model, incorporating key recommendations from subject matter experts in payment model design and health equity intended to strengthen health equity in APM design and implementation, regardless of geography. The payment model is comprised of three key elements: direct patient care payment, population health payment and performance-based payment.
Recommendations to Advance Equity
Element 1: Direct Patient Care Payment
- Transition from fee-for-service (FFS) to capitated payments. Health Plans and other stakeholders working to develop APMs should consider gradually transitioning from FFS to capitated payments to provide upfront funding for clinical services and key staff roles, addressing social factors influencing health and advancing equity. Incremental approaches, such as phased strategies and tracking provider preferences, can facilitate a smooth transition.
- Incorporate risk adjustments for PMPM. Adopt risk adjustment into APM contracts, acknowledging the underlying clinical and social risk of the population. This ensures that reimbursements account for higher-risk populations, recognizing the need for additional resources to eliminate health inequities. Clear goals and method determination are essential in building an effective risk adjustment strategy.
Element 2: Population Health Management Payment
- Incorporate a distinct population health management payment. Separating the population health management payment from patient care payments supports practice improvement, especially for historically under-resourced providers serving populations experiencing health inequities. Payments can be tied to specific activities, with requirements related to the promotion of health equity, fostering targeted interventions and support.
- Provide technical assistance. Effective technical assistance should be offered to providers, encompassing guidance and support for culturally and linguistically appropriate quality improvement interventions. Tailored technical assistance can facilitate the integration of community-based providers, ensuring alignment with health equity goals.
Element 3: Performance-Based Payment
- Weight quality-based payments to equitable health outcomes. Develop financial incentives that meaningfully reward the reduction of health disparities and promote equitable health outcomes. Establish improvement and attainment goals with expectations for data stratification by race and ethnicity. Incentives should align with measures required to be stratified by national and state governing bodies, fostering a focus on equity performance.
APMs, with intentional design considerations for health equity, can uniquely contribute to addressing health disparities. Direct investments and dedicated support are crucial elements, ensuring that practices serving rural or underserved areas have a viable path to success within the payment model. Multi-stakeholder alignment and ongoing collaboration are key to driving cooperative changes and improving the delivery of care. The journey toward APMs requires collective efforts and guidance from diverse stakeholders, from payers and providers to community-based organizations and those receiving care.
For a more detailed look at the recommendations, read our latest issue brief.
Advanced Primary Care Key to Reducing Health Inequities
June 14th, 2023
Robust, comprehensive primary care – a critical foundation for a more cost-effective, high-functioning health system – is equally important in helping boost health equity, a new report states.
The report, produced by the California Health Care Foundation, underscores the variety of ways in which advanced primary care can advance equity in care access and quality for underserved populations. Yet it also warns of significant barriers that continue to thwart primary care’s potential in California and nationwide.
In the face of these obstacles, employers can take steps today to strengthen primary care and reduce health care inequities. Actions can include expanding primary care locations, pushing insurers to strengthen financial support for primary care and increasing telehealth capabilities.
Unlocking Health Equity through Advanced Primary Care
Long-standing racial and economic discrimination in health and social policy has fostered pervasive health gaps for people of color. These disparities range from greater disease burdens and more mental health problems for racially minoritized populations to increased mortality and shorter life expectancies. Historically marginalized racial and ethnic groups also contend with less insurance coverage and reduced access to care.
The good news is that the key components of advanced primary care are particularly well-suited for reversing systemic health care inequities, according to the California Health Care Foundation report. Primary care’s capabilities and resulting benefits include:
- Improved access: A higher density of primary care physicians has been repeatedly linked to increased preventive services, lower avoidable morbidity and mortality and longer life expectancy among Black populations. Increasing the supply of diverse primary care doctors also helps reduce racial disparities in referral patterns and increases needed hospital care for Black Americans.
- Improved care continuity: Ongoing, individualized care provided by a single primary care clinician or practice is tied to lower mortality rates and fewer disparities in receiving recommended cancer screenings among Black and Latino populations. Interpersonal continuity with a primary care practitioner likewise enhances patient trust, which translates into better adherence to recommended preventive services, treatments and medications.
- Better coordination of care: Continuity across provider types and health care settings is shown to reduce racial and ethnic inequities in many important areas, including preventable emergency department visits and improved blood pressure control. For patients with multiple chronic conditions, coordination also lessens the burden of interacting with a fragmented and disorganized care system.
- Greater comprehensiveness: Integrating behavioral health and primary care services is considered one of the most effective ways to improve mental and physical health outcomes while eliminating inequities in care quality and access for racial and ethnic minority populations.
- Whole-person orientation: Elements of accountable, whole-person care — including clinician knowledge of a person’s overall medical history, social needs, preferences, family and cultural beliefs — improves patient self-management for chronic conditions. This is important for patients from racially and ethnically minoritized groups, who are more likely to suffer from complex comorbidities.
Advanced primary care’s power to mitigate health inequities highlights the wider benefits it can produce. Adults who regularly see a primary care physician have 33% lower health care costs and reduced odds of dying prematurely than those who see only a specialist. Every $1 increase in primary care spending produces $13 in savings.
Despite these critical advantages, primary care remains woefully under-resourced, accounting for 35% of health care visits yet only receiving 5.4% of all spending on health care in the U.S. Reimbursement for Medicaid services for low-income, at-risk populations is significantly less than Medicare and commercial rates. As a result, many young doctors burdened with student debt opt for better-paying specialties, exacerbating an already severe primary care clinician shortage.
Employers Can Take Steps to Bolster Primary Care and Advance Health Equity
Notwithstanding these challenges, employers can take steps today to accelerate advanced primary care to help reverse inequities and improve overall employee health, including:
- Increasing the overall proportion of funds dedicated to primary care. Ask your health plan what percentage of spending currently goes to primary care and work to develop incremental increases over time. To track health plan performance over time and hold plans accountable for performance, more than two dozen members of the Purchaser Business Group on Health have signed onto a first-of-its-kind tool called the Health Value Index, which creates actionable insight into a purchaser’s health plan spending and incentivizes both short- and long-term improvements in care for participating companies’ employees.
- Request data on self-identified race and ethnicity, sexual orientation, language preference and disability status: Ask providers and plans to report their REaL (Race, Ethnicity and Language) and and to identify how they’re working to address health care inequities. With this data you can also begin to identify gaps in equity among your employees and families. Some easy places to start is stratifying primary care spend and use of a primary care clinician by REAL data to identify gaps to focus on within plan design. This work is difficult, so it could require engaging with experts to help you develop and apply a shared structural understanding of racial inequities to ensure that your team is generating accurate, helpful and actionable insights from data analysis.
- Ensuring access to telehealth that is coordinated with primary care. Telehealth has emerged as a critical tool for advancing health equity by increasing access for underserved populations. Employers should ensure that telehealth services are available for employees, as well as go one step further by working with vendors to ensure that telehealth services are coordinated with the employee’s primary care physician. When telehealth is a service provided by the primary care clinician, this coordination is already in place, however there are many third-party vendors offering telehealth services and employers should be thoughtful in terms of mitigating the risk of creating a two-tiered system that contributes to fragmentation of care.
- Adopting a holistic approach to employee health benefits. Employers should work with their plans to ensure collection and identification of social risk factors and needs that could be affecting their employee population. This would allow for holistic benefits design that could provide assistance to employees with addressing social needs that can have negative, long-term impacts on employee health.
- Ensuring adequate mental health resources. Ideally, behavioral health capabilities should be integrated with primary care to increase access and whole-person care. Setting this expectation for health plans and providers as a purchaser, as well as increasing investment into primary care to ensure these services can be funded, will help ensure these resources are prioritized and funded.
- Expanding after-hours primary care access. There are multiple models supporting after-hours care, including use of telemedicine or expanding clinic hours. Ultimately, purchasers must champion payment reform that will make these types of services possible. Much like with mental health, employers can support this conversation by also highlighting after-hours primary care access as an expectation that this is a part of critical infrastructure and including it in the purchase and payment of services.
Transforming Health Care Through Primary Care
Given advanced primary care’s unmatched ability to both address inequity and transform our health system, consensus is building around efforts to overcome longstanding financial barriers and dramatically strengthen the nation’s primary care infrastructure.
The California Health Care Foundation report, for example, calls for a new paradigm that includes programs to increase recruiting and training of primary care physicians, increased primary care spending, improved Medicaid reimbursement and expanded primary care hours and locations. Employers can play an essential role in pushing payers to invest in primary care, as well as encourage providers to use the investment to realize and extend the many benefits advanced primary care offers.
Ultimately, it is about increasing equal access to high-quality primary care for all. Having access is equity.
Special thanks to Rishi Manchanda, M.D., co-author of the CHCF report.
Better Data Collection Essential to Understanding and Addressing Health Inequities
December 14th, 2022
The COVID-19 pandemic exposed and exacerbated the weaknesses of the U.S. health care system and highlighted long-standing inequities for minority communities. Highlighted during this period was the profound impact of economic stability, education, social and community life, one’s neighborhood and access to high-quality health care—social determinants of health—on the overall health and well-being of communities.
As a result, addressing health inequities has become a top priority for many employers, purchasers and health care providers. The ability to effectively collect a range of data points about patients and the care they receive is an essential component to creating meaningful change and ensuring populations achieve their full health potential.
Looking at health quality data by race, ethnicity, language and other patient characteristics, is crucial for understanding how long-standing systems of privilege and oppression impact the health of minority populations and communities. However, patient self-reported race, ethnicity and language (REaL) data across health insurance markets is widely variable and overall limited. While race and ethnicity data in California’s Medicaid program (called Medi-Cal) is broadly available likely because of legislation requiring health plans to collect this information starting in 2009, corresponding data for the majority of patients who receive health benefits through the commercial market – via employers or on the private market –is low or absent.
These limitations of known race and ethnicity data hinder the ability to see where disparities exist and for the health system to react with meaningful interventions. For health plans and large employers and purchasers, who provide health benefits for more than half the U.S., it is crucial to uncover variation in the access to care and the quality and experience of care being provided.
With better self-reported patient demographic information, employers, purchasers, payers and providers can tie this data to health care access, quality, patient experience and outcomes to illuminate exactly where disparities exist. These insights can enable tailored interventions and support for improvement.
How to Improve Data Collection
Legislation, Policy and Regulation
Legislation and regulations can incentivize or require health plans, providers and other health system organizations to increase the collection and quality of self-reported demographic data. Legislation and statute also have the potential to enforce standardization for data fields and definitions, which enables largescale purchasers of health care to align with their health plan and provider industry partners and enhance their ability to share, aggregate or disaggregate data to identify trends and implement plans for improvement.
It is crucial to ensure that national and state standards do not contradict each other.
Contracting and Business Relationships
Contracting requirements and incentives as part of large-scale public and private purchaser and payer programs can increase the collection, reporting and use of REaL data and thereby bolster efforts to mitigate disparities. Large purchasers could add incentive payouts if plans are able to stratify measures across self-reported REaL data. Health plans, provider organizations and other payers that contract within the health system can use incentive payouts for better data collection and stratification and other efforts to reduce disparities. Another approach is to build tiered networks that point patients to providers who have proven to be stronger at collecting, reporting and using REaL data.
It is important for purchasers and payers to avoid siloed initiatives that conflict with each other.
Organizational Leadership, Systems Structure and Culture
Organizations that pay for services at the point of care (e.g., health plans and independent physician associations, or IPAs) have the potential to increase REaL data collection, reporting and use by assessing and enhancing data collection opportunities, sharing data internally and creating a culture that values the collection of this information. This starts with organizational leadership. It is important to normalize data collection into regular workflows to improve the quality and ensure the most accurate information possible.
Purchasers, health plans and provider organizations can increase patient self-reporting by increasing awareness of how the data will be used and educating enrollment counselors and other staff with direct patient interaction on why it is important to collect this data.
Certification Requirements
The National Committee for Quality Assurance (NCQA) has required plans to report their percentage of self-reported REaL data for certain key measures, with a goal of 80% self-reported data. Additional accrediting organizations, purchasers and others could adopt similar certification requirements to support reporting and stratification for the same measures and self-reported data goals as NCQA. This would increase the consequences for not aligning and support the overall goal of greater availability of self-reported REaL data.
Read more in our latest issue brief.
Opportunities in COVID-19 Vaccine Access and Equity
May 4th, 2021
While COVID-19 vaccine eligibility has expanded and supply has increased, data show that access to vaccines are not equitable throughout California’s communities.
Health care leaders are looking to work together differently as their vaccination efforts shift from trying to meet demand through mass vaccination sites to targeted interventions that address the needs and concerns of high-risk communities and vaccine-hesitant individuals.
In late April, PBGH’s California Quality Collaborative (CQC) hosted a closed roundtable discussion for health plans, provider groups and California state agency representatives to discuss challenges and success stories in their efforts to distribute COVID-19 vaccines and support equitable vaccine distribution for under-resourced populations. Five key actions stakeholders need to take emerged from the conversation:
1. Invest internally in policies supporting equity. During the past year, many organizations worked to improve internal processes that would better enable them to serve the diverse needs of their members and staff. L.A. Care Health Plan, the nation’s largest public health plan with nearly 2.2 million members, for example, developed a set of more robust internal policies to address diversity and inclusion, as well as programs designed to minimize barriers in working with minority or women-owned businesses, an approach described in the Clinical Improvement Network Connections spring 2021 publication.
2. Facilitate real-time data sharing. All groups agreed that, while there had been investments in data-sharing that facilitated collaboration to distribute and ensure access to vaccines, there were still gaps between health care delivery systems, public health and community-based organizations in terms of the accuracy of, and timeliness with which, essential clinical data was shared. As we begin to recover from the pandemic work should be done to ensure real-time data-sharing, especially between the California Immunization Registry and health information exchanges and organizations not traditionally part of health care information exchanges.
3. Provide clear, consistent and trusted communication. It was extremely important for all entities to streamline, test and regularly deliver communications campaigns to stakeholders, including community members, provider groups and member patients.
4. Leverage trusted relationships from primary care providers. Primary care providers were unable to play a significant role in the early days of vaccine distribution, often because mass vaccination sites were prioritized so individual practices received limited vaccine supply or were unprepared to accommodate the stringent storage requirements. With vaccine distribution having stabilized, there is an opportunity to tap into the primary care provider community, which is positioned to leverage long-standing patient relationships and play an important role in vaccination efforts. Increasing primary care’s role in COVID-19 vaccine administration may prove extremely effective in reaching vaccine-hesitant or skeptical patients.
5. Sustain new and strengthened partnerships. Overall, there was a recognition that the public health emergency and response has illuminated how effective cross-sector collaboration between health plans, public health departments, provider groups and community-based organizations can be at solving urgent problems when working together. Now, there is a question about how partnering groups can continue to collaborate while finding ways to become more efficient.
COVID-19 Vaccine Resources
Addressing Social Determinants of Health Essential to Reining in Health Care Costs
January 11th, 2021
Health care’s exorbitant costs can never be controlled without fundamentally shifting society’s focus toward the underlying social and economic conditions that disproportionately contribute to ill-health. That was the message former Centers for Medicare and Medicaid Services (CMS) Administrator Donald Berwick gave to large employer members of the Pacific Business Group on Health (PBGH) during a January 7 webinar.
“I’ve lost patience with marginal change. I don’t think it’s going to work,” said Berwick, a pediatrician who led CMS for a year-and-a-half during the Obama administration and who has been a leading voice for health care reform for over four decades. “We continue to confiscate resources in health care that we don’t deserve and aren’t using properly from other sectors that badly need those resources. It’s time for some big thinking.”
The Shadow of Racism and Poverty
In a presentation subtitled “The Moral Determinants of Health,” Berwick hammered home the need to tackle systemic issues like disparities in income, education, food access, housing security and community structure. He pointed to extensive and long-standing evidence showing the outsized impact these factors have on care access, outcomes, health status and ultimately, cost.
In one example, Berwick noted that individuals who’ve been subjected to at least four adverse childhood experiences (ACE) face dramatically higher risks for nine out the top 10 leading causes of death in the U.S. They’re also 10 times more likely to experience mental illness and 11 times more likely to suffer from Alzheimer’s disease, he said. ACEs can include experiencing violence, abuse or neglect, witnessing violence, or living in a household with substance misuse, mental health problems or parental separation due to incarceration.
The COVID-19 pandemic has both exposed and exacerbated the country’s long-standing health inequities, he noted, particularly as they relate to people of color, with black Americans dying of the virus at a rate three-to-four times higher than whites.
‘Fixing the Road’
According to Berwick, unless efforts are made to move upstream to address social and economic challenges and reallocate a portion of the dollars now flowing into health care toward housing, education, food, criminal justice reform and the like, rising costs and widening disparities will continue to be hallmarks of the U.S. health system.
Berwick went on to outline his personal vision for health care transformation in the U.S., components of which include making health care universally available. He also stressed other priorities, such as ending hunger and homelessness, restoring American leadership on climate change and restoring the credibility of democratic institutions.
He noted that PBGH has been an “extremely important force and presence” in efforts to reform health care for decades and applauded the organization’s willingness to engage seriously in pursuit of solutions. Nonetheless, he said, employers generally have largely remained “bystanders” in efforts to address the social determinants of health and challenged purchasers to consider how they can affect change.
“You’re concerned about your health care costs as an employer and the costs for your employees, so connect the dots,” he said. “With 18% of our GDP and $3.5 trillion a year, health care is running a repair shop. But nobody’s fixing the road.”
The webinar, which includes a panel of health care purchasers sharing their organizations’ approach to addressing social determinants of health can be viewed in full below.
Presentation
{kind=link}